
Kay Kay Lineweaver’s first birthing experience in 2021 didn’t go as planned. Her baby was breech and the doctor wouldn’t allow her to try to give birth vaginally, so she ended up with an unwanted cesarean section.
“[The obstetrician] wouldn’t even give me the option,” she recalled later in a podcast called “Healing Trauma Mamas.” Lineweaver said she felt like she “didn’t have control” and that the birth process was “a nightmare.”
Six months later, when she found out she was pregnant with her second baby, Lineweaver was committed to having a vaginal birth after a C-section, or VBAC. That meant there was a relatively small but increased chance that, during delivery, the scar from her prior surgery could tear and her uterus could rupture — a potentially life-threatening event for both her and her baby.
She said hospitals near her home in Abilene, Texas, told her they would only perform another C-section, and a local birthing center wouldn’t accept her.
Lineweaver then looked for a midwife to attend her birth at home, and after receiving several rejections, ended up finding not one but three midwives who were willing. She chose one nearly 200 miles away in Waco, Texas, who had the most experience with VBACs and was near a hospital in case anything went wrong. Lineweaver’s daughter, Nova, was born Aug. 29, 2022, into what she described to STAT as a “calm” environment, in contrast to the hospital birth with her first child.
“I’m a big believer that how you’re brought into this world kind of plays into the person that you become,” she said.
While home births make up less than 2% of all births in the U.S., more and more people are opting to give birth outside the hospital setting, even when they have high-risk pregnancies, according to an analysis of data from the Centers for Disease Control and Prevention.
In 2022, the most recent year for which complete data are available, there were 46,183 home births, a 56% increase since 2016. These home births were planned as such — they were not surprises — and the vast majority were attended by midwives.
The increase in home births was particularly steep during the worst of the pandemic, when mothers may have feared contracting Covid-19 in the hospital or didn’t want to go through labor alone due to hospital restrictions.
During this same time period, high-risk home births, such as Lineweaver’s VBAC, also increased dramatically.
High-risk home births “used to be really underground,” said Ida Darragh, executive director of the North American Registry of Midwives. But now, “there is a community of women who feel that they are going to make their own decisions. They’re educated, they know what the pros and cons are, and they feel that the final decision is theirs on what types of risk to accept.”
Sarah Little, a maternal-fetal medicine physician at Beth Israel Deaconess Medical Center, said the increase in higher-risk home births “raises my concerns.”
In its guidance on home births, the American College of Obstetricians and Gynecologists (ACOG) states that while home births are associated with fewer interventions, such as inductions and C-sections, they also carry a higher risk: The ACOG guidance says that for every 1,000 home births, 3.9 babies will die, which is about twice the risk of hospital births.
ACOG adds that while it “believes that hospitals and accredited birth centers are the safest settings for birth, each woman has the right to make a medically informed decision about delivery.”
The group specifies that three particular situations — VBACs, pregnancies in which the baby is not in a head-down position, and pregnancies with twins or other multiples — are “an absolute contraindication to planned home birth.”
“The reason we called out these three is that the risk is unpredictable. Things can happen quickly, and you need to react,” said Little, a member of ACOG’s Committee on Obstetric Practice, which wrote the group’s guidance in 2017. “They can have some tragic complications, and they’re potentially avoidable with easy access to an operating room.”
VBACs in particular are increasingly common in the U.S. Nearly one-third of births in the U.S. are by C-section. Among women who have a C-section and then give birth again, 14.6% have vaginal births, a percentage that has slowly but steadily increased since 2016.
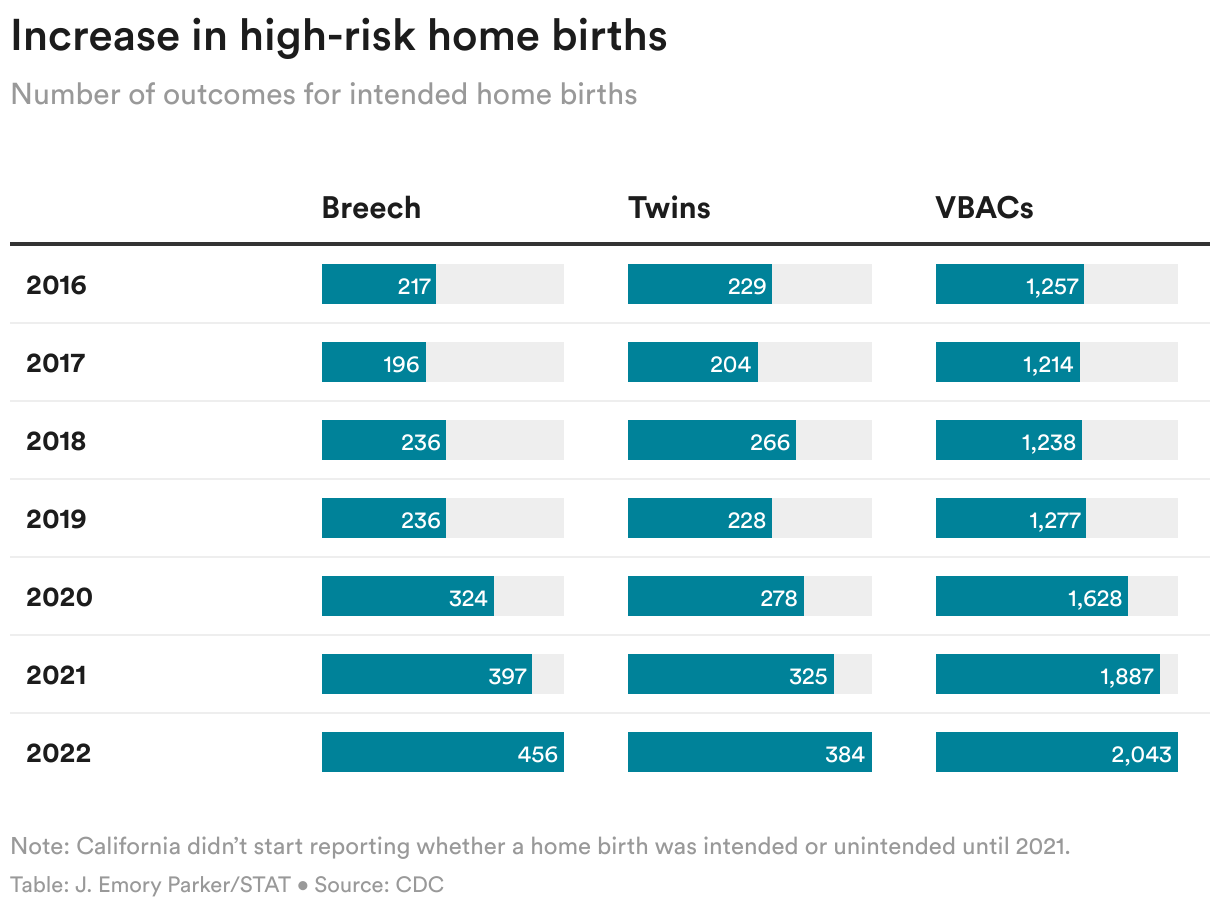
Increase in high-risk home births
The number of home births in the three high-risk situations called out by ACOG — VBACs, breeches, and twins — are still relatively small, but have increased dramatically in recent years.
In 2016, the earliest year for which there is data, 1,257 babies were delivered at home to mothers who’d previously had a C-section. By 2022, that number increased by 63% to 2,043.
In 2016, 217 babies who were born in the breech position were delivered at home. By 2022, that number more than doubled to 456.
And in 2016, 229 babies who were twins were born at planned home births, and by 2022, that number increased 68% to 384 babies.
There’s not a lot of data specifically focused on the safety of high-risk home births. A 2015 study that looked at trials of labor — that is, attempts at vaginal birth — for mothers in the U.S. with a previous cesarean found that for every 1,000 home births, there were 4.75 fetal deaths. Trials of labor at U.S. hospitals have a fetal death rate of 0.13 per 1,000 births, according to a study cited by ACOG. The 2015 study urged that women planning a home VBAC be counseled regarding the “potential for increased risk to the newborn.”
One mother’s decision
During her second pregnancy, Lineweaver read the 2015 home VBAC study, and many more.
“It became my full-time job, essentially, to read the research, understand my true risk, [and] understand if I was making the right decision,” she told Midon Wingo, host of the podcast “Healing Trauma Mamas,” that was published last September.
Lineweaver said she felt comfortable with the increased risk for two reasons.
First, she found the certified professional midwife three hours away in Waco who had years of experience with home VBACs. Lineweaver and her husband, Tyler, had several discussions with the midwife about the risk of a uterine rupture and how they would go to the hospital if something went wrong. A few weeks before her due date, the family drove from their home in Abilene to an Airbnb in Waco so they would be near the midwife when Lineweaver went into labor.
Secondly, if anything did go wrong, the Airbnb was 10 minutes from a hospital.
While the Lineweavers awaited their temporary move to Waco, Sabrina Elliott, a licensed and certified professional midwife in Abilene, provided prenatal care.
Elliott, vice president of the Association of Texas Midwives, said she screens potential clients carefully to make sure they understand the benefits and risks of a home birth. She said Lineweaver “had done so much of her own research, and that’s usually what I look for — not somebody who’s just like, ‘Oh, I’ve heard that this is a thing and I want it.’ I want to know that you already know the statistics.”
One particular statistic in the 2015 VBAC home birth study caught Lineweaver’s eye. She was committed to avoiding a C-section if possible, and that study showed that the majority of the women in the study who attempted a home VBAC — 87% — ended up having a vaginal birth.
She said a “bonus” reason for giving birth outside a hospital was that she wanted a positive experience not just for her daughter as she entered the world, but for herself, too.
In the end, Lineweaver got what she wanted.
“It was probably the most magical, spiritual, just kind of renewing type experience I’ve ever had,” she said. Immediately after giving birth to Nova, “it was like ‘I’m ready to have another baby,’ which sounds crazy, but it was such an amazing experience.”
But Little, the ACOG committee member, said she worries that a birth like this could have gone the other way.
Little, who is also an associate professor of obstetrics at Harvard Medical School, said that when she does trials of labor for women who’ve had previous cesareans, she’s right next to an operating room. She said she worries that being even just 10 minutes away from a hospital would be too far in the case of an emergency.
“With a uterine rupture, the only thing you can do is get to the OR,” she said. “You wouldn’t even want to be next door to a hospital.”

Lack of trust in hospital care
Eugene Declercq, a childbirth researcher, isn’t surprised by the increasing trend in home births.
A professor at the Boston University School of Public Health, Declercq is part of a team that publishes a series of surveys called “Listening to Mothers.” In a 2016 survey of more than 2,500 new moms in California, 22% expressed interest in making their next birth a home birth. That number was particularly high for Black mothers, with 29% expressing an interest.
“This is about dissatisfaction with care at the hospital. This is about a lack of trust in that care,” he said.
Declercq is also co-author of a 2019 study that surveyed more than 2,000 U.S. mothers of young children about experiences with mistreatment during childbirth — for example, being shouted at, scolded, or receiving no response to requests for help. In the survey, conducted in 2016 and 2017, 28% of women who gave birth in a hospital reported mistreatment. Among those who gave birth at home, 5% reported mistreatment.
In that study, white women were the least likely to report mistreatment — 14.1%, compared to 22.5% for Black women, 25% for Hispanic women, and 32.8% for Indigenous women.
A recent CDC report on mistreatment among women receiving maternity care highlighted a similar pattern, with 30% of Black women reporting mistreatment compared to 19% of white women.
Studies show that systemic racism makes hospital births especially risky for Black women, meaning that this group in particular may have safety concerns about giving birth in a hospital system. A 2023 Journal of the American Medical Association study found that maternal mortality rates for Black women more than doubled between 1999 and 2019, reaching an average 67.6 deaths per 100,000 live births in 2019.
While the number of Black women who opt for home births is still small, the increase in home births has been particularly steep. In 2016, 823 Black women gave birth at home. That number more than tripled in 2022, to 2,733. In 2016, 50 Black women had VBACs at home, and that number more than tripled in 2022 to 153.
Cassaundra Jah, executive director of the National Association of Certified Professional Midwives, said she worries that some people, of any race, might be so dissatisfied with their hospital birth that they then seek out a home birth without first researching what risks they might be facing.
“Many times, especially in VBAC situations, clients have had disproportionately traumatic first births, ending in surgery,” said Jah, a midwife in Austin, Texas, who has attended many home VBACS during her 14 years in practice. “But really they’re more choosing not to have that experience again than they are actively choosing to have a home birth.”
Declercq said two changes would increase safety for women in high-risk situations such as VBACs, breeches, and multiples.
First, hospitals should improve their care, including providing more training for staff, so that fewer women suffer mistreatment, making them less likely to avoid hospital births in future high-risk situations.
Second, for women who choose home births, arrangements could be made that allow for more seamless transfer to hospitals if something goes wrong, and without fear that staff there would criticize the mother and the midwife for trying a home birth.
In countries that have such arrangements, such as the Netherlands, home births have better safety records than in the U.S. Washington state also has arrangements in place that allow for rapid and easy transfer to hospitals, and home births there have similar safety rates as accredited birthing center births, according to a 2021 study.
“That study shows us how good home birth can be — how safe home birth can be under the right circumstances,” said Kate McLean, an obstetrician and former chair of Washington’s ACOG chapter. “This should motivate all of us to get medical systems in place to support home birth and integrate it within the community so home birth can be this safe anywhere.”
McLean said while there isn’t enough data to support anyone having a high-risk birth at home, there’s a reason that people from marginalized backgrounds, concerned about the care they may receive in hospitals, might opt for a home birth even with a complex pregnancy.
“If they have the option for culturally congruent care with a competent midwife in a home birth, I think it’s very understandable that they would want to take it,” McLean said. “We here in the United States really need to do better.”
This story is part of ongoing coverage of reproductive health care supported by a grant from the Commonwealth Fund.
To submit a correction request, please visit our Contact Us page.










