
A panel of government advisers finally has endorsed ideas for Congress to solve the particularly thorny problem of surprise ambulance bills, including a cap on how much patients would have to pay if they took an ambulance.
Surprise bills have been eliminated for most health care services, but people who take out-of-network ground ambulances remain broadly unprotected — facing potentially thousands of dollars and the threat of collections for a ride that nobody really asks for.
Most notably, members of the ambulance committee agreed last week during a two-day meeting that patients should not pay more than $100 out of pocket for any emergency ride, a decision that could provide the most tangible relief yet. But there was much less consensus around figuring out how much ambulances should actually get paid. The federal committee, which is primarily composed of people who work in the ground ambulance industry, ultimately embraced policies that allow ambulance providers to set their own rates — raising concerns about whether the solution will lead to runaway costs.
“It’s just poor public health to have question marks in people’s heads about the cost of calling an ambulance,” said Patricia Kelmar, senior director for health care campaigns at the consumer advocacy group U.S. PIRG. By at least endorsing a maximum of $100 for any emergency ambulance ride, “it gives certainty, and it is a somewhat manageable amount.”
Figuring out how to pick up the tab for ambulances will be a national experiment, if and when Congress decides to put the committee’s recommendations into law. A new collaboration from STAT and the health policy podcast Tradeoffs explores how the potential solutions could pan out, based in large part on the experiences of other states that have already tried to fix the issue somehow.
Currently, payment disputes between out-of-network providers and insurance companies for services other than ambulances go through a federal arbitration process that has been nothing short of a clogged-up mess. For ambulance disputes, resolutions are arguably even messier. They usually result in insurers and employers paying what they think is fair, and then ambulances chase patients for the balance and haggle with insurers to try and get more money.
Instead, the ambulance committee recommended Congress find another way that offered more predictability for each party, specifically by instituting a form of rate-setting.
Ambulances and insurers would first defer to the 14 states that have some kind of ambulance surprise billing law on the books. If that doesn’t apply — for example, if a patient is enrolled in a federally regulated employer health plan — payments would be based on locally set rates that must go through a public process but contain no upper limit on how high they can be set. If there is no locally set rate, payments would be based on a percentage of Medicare set by Congress.
Those types of rate-setting arrangements — as when local governments determine payments, or when payouts are pegged to some percentage of what Medicare already pays — each have benefits and drawbacks.
Some experts say a Medicare benchmark is the simplest administrative solution. Medicare’s payment system for ambulances is outdated, but it’s based on some measure of costs. But that shift would result in a lot of upheaval, especially for ambulance providers that currently are able to bill and collect large sums of money from the biggest insurance companies.
“The variation in the commercial payments that I see suggests that almost whatever level [would be picked as a Medicare benchmark], there’s going to be significant winners or losers,” said Zach Gaumer, a former analyst at the Medicare Payment Advisory Commission who is now a consultant at Health Management Associates.
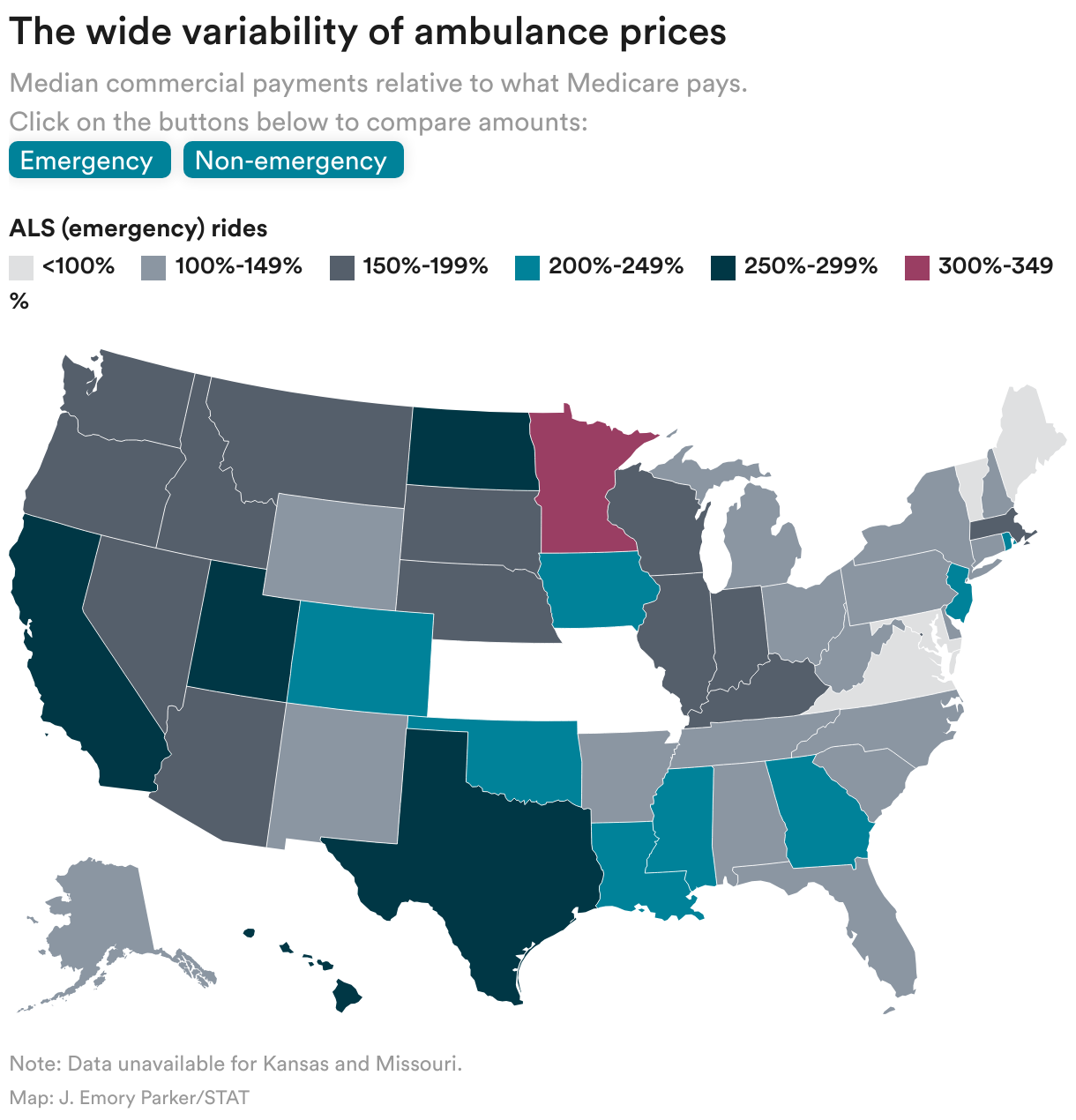
For example, in Minnesota, the median amount that a commercial health insurer pays for an emergency ambulance ride is at least 300% of what Medicare pays, according to Gaumer’s analysis of ambulance claims data from FAIR Health, a nonprofit group that analyzes health care data. Payments for non-emergency ambulance rides are higher for even more states. However, the median amounts insurers pay for emergency rides in four states — Maine, Maryland, Vermont, and Virginia — are less than 100% of Medicare, meaning ambulance providers in those states would greatly benefit from a higher percentage of Medicare.
Colorado has instated a limited version of paying ambulances a percentage of Medicare. Publicly run ambulances in Colorado were exempted from the law that paid 325% of Medicare. Those ambulance agencies were fearful that relatively high rate still wouldn’t be enough. But Adam Fox, deputy director of the Colorado Consumer Health Initiative, said the law has garnered support because it still guarantees payments.
“The underlying structure from our perspective works much better if there is a benchmark reimbursement that the ambulances can count on that protects the consumer and ensures that we’re setting reasonable costs,” Fox said.
Relying on local governments to set out-of-network ambulance prices would create a separate kind of upheaval — one that could potentially lead to higher premiums for the insured and create the same kind of conflicts of interest that exist within Medicare’s system for physician payments. It’s also not clear those governments are up to the task.
“There’s great administrative burden in doing this,” Gaumer said of locally set ambulance rates. “And I’m not so sure that I can see the smallest counties in America being able to do this.”
Emergency medical groups viewed locally set rates as a compromise that importantly would delegate and keep power in municipalities and counties. And at least four states recently passed laws that require insurers to honor locally set rates for out-of-network ambulance providers. Most are Republican-leaning states like Arkansas, Louisiana, and Texas, where raising taxes for ambulances would be especially unpopular.
Supporters of local rate setting argue there’s a natural check on this method: a public process people can weigh in on.
“Local communities aren’t just going to go willy-nilly and raise rates to take advantage,” said Butch Oberhoff, president of the Texas EMS Alliance. “They’re still accountable to constituents. They would have to explain why they raised rates.”
That leap of faith will be put to the test again next year, when California starts to require insurers to pay out-of-network ambulances according to locally set rates. That price-setting process is public, but some advocacy groups still worry costs could rise considerably without clearly defined caps or ceilings on what can be charged.
“We’ll have to pay attention and make sure [ambulances] don’t use this as an incentive to raise the rates,” said Jenn Engstrom, the director of California PIRG, a state offshoot of the national consumer advocacy group. “If things skyrocket, we’ll need to see if we have to take action and do something different.”
Early next year, the federal ambulance committee will deliver its recommendations to Congress. Key lawmakers have not shown a lot of interest in taking up surprise billing again because it requires a lot of political capital to confront the ambulance and insurance industries.
“We’re going to be pushing Congress. It will be hard. There will be people who won’t like it,” said Kelmar, a member of the federal committee. But she thinks there is a clear pitch that could interest Congress to act.
“We are guaranteeing a payment to our ambulances, which right now is not happening,” Kelmar said.
Leslie Walker and Dan Gorenstein of Tradeoffs contributed reporting.
To submit a correction request, please visit our Contact Us page.











STAT encourages you to share your voice. We welcome your commentary, criticism, and expertise on our subscriber-only platform, STAT+ Connect